
Two years ago we asked whether a health/patient advocate can also be a decision-maker for her client in the form of being a healthcare proxy or guardian (the patient-designated person who makes end-of-life decisions for the patient, based on wishes the patient has legally documented). Since the ethics and standards of the original advocate role very specifically state that an advocate WILL NOT and CAN NOT make decisions for a client, would the new role of proxy or guardian create a conflict-of-interest?
The scenario shared was that “Gwen” had been Mrs. Smith’s advocate for a long period of time and they had developed a close relationship. Mrs. Smith, at the age of 90, wanted Gwen to be her healthcare proxy to help determine (if necessary) when it was time to allow Mrs. Smith to die, instead of conceding to the healthcare system’s attempts to keep her alive at all costs.
Could those two roles be performed by the same person? We didn’t answer the question. Instead, we used the opportunity to develop a best practice by asking for input and opinions from those in practice at the time. The question:
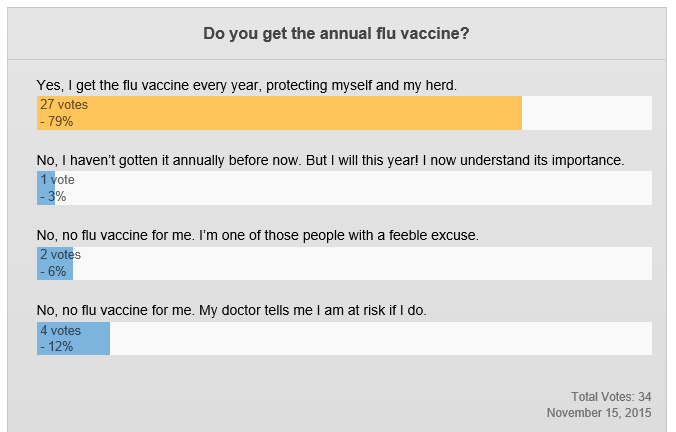
Should Gwen become Mrs. Smith’s healthcare proxy? Can she ETHICALLY make that shift?
And the results were… (drum roll please!)….
409 total votes:
> 211 agreed that Gwen can ethically be Mrs. Smith’s healthcare proxy
> 198 said that no, she cannot ethically make that shift
Fast forward to 2016 when the question was asked again. Only this time it was not a fictional scenario. It was a question that came to us from a member of the Alliance about a real potential client.
This time the client (we’ll call him Mr. Sanchez) is in his late 60s, single with no family, few friends (who he believes will die before he does), and a family history of stroke. Mr. Sanchez wants to find an advocate to help him develop his end-of-life wishes and documents, then be the person who carries them out by making decisions for him when the time comes.
The advocate’s question to APHA: does this create a conflict-of-interest? (We should note that Mr. Sanchez could not understand the potential conflict. After all, if the advocate was only carrying out the decisions he had made originally, wasn’t she just doing what he had hired her to do?)
Understanding better the issues raised when the question was asked in 2014, and with the ensuing development of the Ethics Statement by the Patient Advocate Certification Board (PACB – the group developing patient advocacy certification) we checked in with Steven Okey, an attorney, our APHA Legal Advisor, and president of the PACB, for his thoughts on the topic.
- Read: The Ethical Standards developed by the PACB
Here is Steve’s analysis:
Being aware of the potential conflict of interest is the beginning of the analysis, but not the end. If this scenario does present a conflict of interest which is subject to reasonable debate then it’s important to remember that a client can waive a conflict of interest.
The 6th Ethical Standard of the Patient Advocate Certification Board states in pertinent part:
A conflict of interest exists when there is a substantial risk that the advocate’s services to a client will be materially limited by the advocate’s personal or professional interests. An advocate shall not start or continue to provide services to a client when a conflict of interest exists, unless both of the following apply:
> (a) the advocate will be able to provide competent and diligent services to the client, and
> (b) the client gives informed consent, confirmed in writing.
As long as both (a) and (b) are met, an advocate can still ethically provide the services sought by the client.
The problem usually arises when an advocate fails to inform the client about the conflict or fails to get the client’s informed consent in writing. If you follow this Ethical Standard, there is likely to be no problem. (Even if an advocate simply ignored a conflict of interest which of course should never be done, that alone would never be enough for an advocate to be found liable in a lawsuit. In every case, the client or the client’s family would have to prove both that the advocate was negligent and that the negligence directly caused injury to the client.)
 Advocacy and proxy decision-making are like oil and water. They most definitely co-exist, but they really just don’t mix.
Advocacy and proxy decision-making are like oil and water. They most definitely co-exist, but they really just don’t mix.
However, the true goal of advocacy is about helping patient-clients transition through their own medical and health situations. So when end-of-life becomes their concern, advocates need to be prepared to provide some sort of response if the question is asked about being both advocate and proxy.
Based on Steve’s response, and the now-available PACB guidelines, here are some steps and solutions you may tap into when the question is asked of you – when your Mrs. Smith or Mr. Sanchez want you to be both advocate and proxy. They represent the side we know – patient advocacy – and the side we will switch to – a form of guardianship.
The goals are to serve your client, conduct business ethically and professionally, and to make sure that no one can second-guess your approach or decisions afterward.
If you are comfortable with representing your work as both advocate and proxy or guardian for the same client:
- Be sure he/she understands the conflict of interest but still wants you to play both roles.
- Work with your client’s attorney to create paperwork for both roles, dated and signed, drawing a distinct line, possibly defining a trigger between the roles. This will not only help the two of you understand the two roles, it will help those nieces and nephews who come out of the woodwork later to better understand once your client dies.
- Consider doing other cover-your-backside things like making a video with your client, or helping your client write a letter that describes how he/she understands your different roles.
- Notify and stay in ongoing touch with anyone else who will be involved before or after your client’s death such as attorneys, heirs, or the executor of his/her will.
- Be sure that when you switch from one role to the other, you nullify the advocacy contract. Connect with the same attorney who helped you draw up the paperwork.
If you are not comfortable with both roles being performed for the same person:
- Find a partner or subcontractor who will take on the role you don’t want to take (If you are the advocate, help the client find someone else to be the proxy, someone who is willing to spend time to get to know the client.)
- Refer the potential client to someone else who will work out the roles. (You can use the AdvoConnection Directory to help find someone who would be competent to help.)

Over time, as baby boomers and ‘elder orphans’ (solo seniors) continue to age, this scenario and this question will become more common. Smart advocates are prepared with their own approach to answering these potential clients’ questions, and providing solutions that work for all involved.
LEARN ABOUT APHA MEMBERSHIP | FIND MORE REASONS PATIENTS NEED ADVOCATES



Very good and helpful article on a topic that will become a regular issue in the years to come.
Today I will draw up an Advance Care Directive for Abi, a client in Sydney Australia. She is the most isolated woman I have ever met. She absolutely hates Mary her sister in Australia and gets on well with Lynne her sister in California. Mary is not to get “even the underwear I die in” when she dies. Her best friend is someone who swims at the local pool at the same time as Abi. She has known her for just a few months. She has no children or other friends and her husband is dead. At this stage she has no will, power of attorney or enduring guardian. She is a retired nurse and knows exactly what she wants and does not want should she become seriously ill. She fears having decisions left to “the system”. Hence the Advance Care Directive.
Her request to me is to a) help her draw up the Directive and b) be available to monitor its execution. My plan is to be available to consult with Lynne about decisions. I am going to avoid deciding anything myself, hard as that will be with Lynne in another country. My experience as an ICU nurse tells me that Advance Care Directives are pretty explicit and detailed. Lynne will have a copy. If Abi becomes ill I will have her treating doctor and Lynne on the phone immediately and they can make the decisions. I will only intercede if I believe Abi’s wishes are not being followed or if her care is sub standard. As an advocate, I see my role as drawing up a very comprehensive document that list me as the primary contact person. Thereafter, I am a collaborator, liaison person, monitor, supporter and record keeper. But there is no purpose in making myself a target.
Trisha, very interesting topic and thank you also to Steve for providing such great perspective. A couple of considerations for anyone faced with this request. One, this client is 67 and may live another 10-20 years. Will your practice be in existence to see through the medical proxy part? And second, what technologies do you need to put in place to help maximize the likelihood that first responders will locate the client’s advanced directive and/or you.
Excellent additions to support both the patient-client, and the advocate, too.
Thanks AnnMarie.
I work with a clientele who are almost all disabled, many intellectually as well as physically. This topic is 100% relevant for them.